
An abnormal position of the head occurs when the eyes are not spontaneously straight, but become straight only by assuming a particular position with the head. The head can be turned sideways (to the right or left), vertically (up or down), or tilted over one shoulder. The patient assumes this position spontaneously or when he wishes to make the most of his sight.
Causes of ocular torticollis
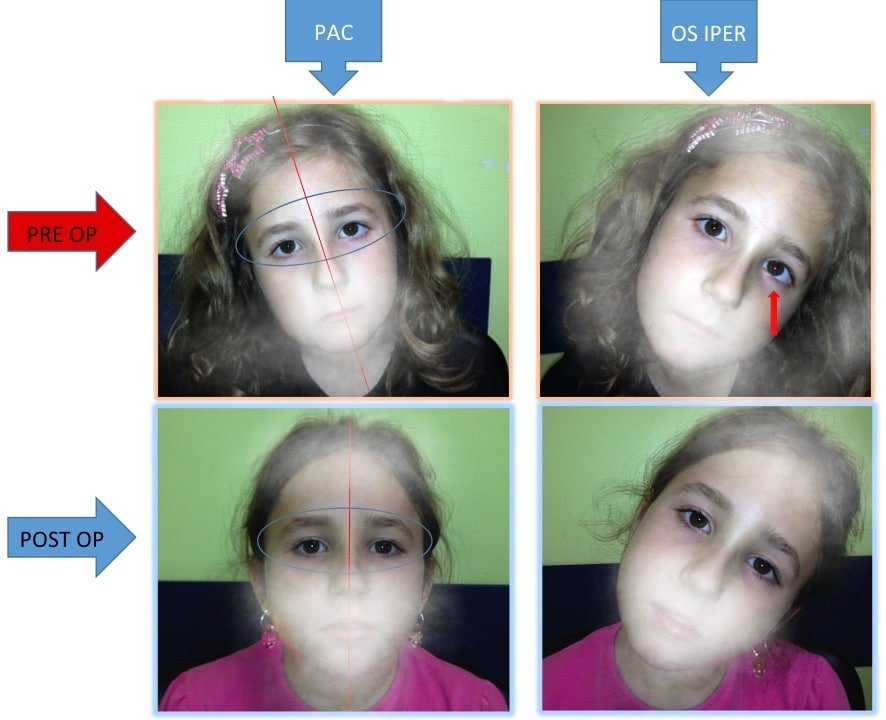
Strabismus: in some cases of strabismus the magnitude of the angle of deviation changes in the various positions of the gaze. The person spontaneously turns his head to where the eyes are mostly straight. Some causes of ocular torticollis are: paresis of the great oblique, Duane’s syndrome, Brown’s syndrome, squinting resulting from fractures of the orbital floor, and hyperthyroidism.
Nystagmus: Some patients with nystagmus assume an abnormal position of the head to put their eyes in the direction in which the nystagmus disappears or reduces.
The child adopts the abnormal head position to try to see with both eyes together (binocular vision), to avoid diplopia (double vision), or to reduce nystagmus by improving visual acuity. It is good to let the child adopt and use the abnormal position of the head but at the same time consult a pediatric ophthalmologist quickly for a precise diagnosis.
Transcript of the video.
Torticollis is an abnormal position of the head that is assumed either due to skeletal or muscular anomalies or in the presence of problems concerning the eye. Torticollis can therefore be characterized by a rotation to the right or to the left, by a so-called elevation of the chin, or rotatory.
In the event that it is related to skeletal or muscular problems, it will be difficult to rotate the head in the opposite direction and this allows us to make a differential diagnosis. We then passively turn the patient’s head to the opposite side of that is usually used to evaluate the anomalies. At that point, you may also consider an ocular problem that may be linked to strabismus, nystagmus, a refractive defect, or the presence of ptosis (lower eyelid).
In the case of strabismus, it is easy. The patient may adopt frequent squinting and stiffer necks because the alignment of the eyes is better in some directions or head positions. The compensatory head posture may allow the patient to have binocular vision and be undisturbed by diplopia.
In the case of nystagmus (continuous oscillation of the eyes), there are certain positions in which this eye movement is reduced or stopped altogether (null point) and therefore allows the patient to see more precisely. Then there are some simple refractive defects such as myopia and astigmatism that are strategically corrected by moving the head and adopting a stiffer neck, so they will simply be corrected with a pair of glasses and then in the presence of ptosis (lowered eyelid), it is often characterized by the presence of a stiff neck with chin moving upwards.
In the case of strabismus, to correct torticollis, the therapy is to surgically correct the strabismus and thus succeed in placing the gaze in the primary position and having the eyes straight. The patient will no longer have to adjust to this abnormal head position in order to use the eyes collectively.